
My career vision is to understand the epidemiology and genetics of childhood rheumatic diseases, specifically juvenile idiopathic arthritis and childhood onset systemic lupus erythematosus.
Juvenile idiopathic arthritis (JIA) is the most common cause of chronic arthritis in children, affecting 1 in 1000 children. Although it was once thought that children with JIA “outgrew” their arthritis it is now clear that a significant number of children with JIA go on to have arthritis as adults. Both genetic and environmental factors predispose to the development of JIA. Our research focuses on identifying genetic factors that predispose to JIA susceptibility. We have assembled a large cohort of cases with JIA and healthy controls. We have also investigated a number of candidate genes for association with JIA and have demonstrated that variants in genes encoding CCR5, STAT4, TNFAIP3, and C12ORF30 are associated with JIA susceptibility. We have demonstrated that siblings of children have a twelve fold excess risk of JIA and first cousins of children with JIA have a six fold excess risk of JIA compared to the general population. We have also demonstrated that children with JIA and their family members are at increased risk of autoimmune disorders in general.We are part of an international consortium on genetics of JIA. We also have a special focus on children who develop rheumatoid factor positive JIA, as this subtype resembles onset of adult RA in children. We have reported on the genetic basis of childhood onset RA.
We are now also focusing on childhood onset of SLE. SLE is a multisystem autoimmune disease that predominantly affects females, and is two to three fold increased in African American children. We are investigating the immunological profile of childhood onset SLE, and also studying epidemiological factors that influence SLE.
SEARCH: South Eastern Registry of Childhood Arthritis
Childhood arthritis refers to a collection of autoimmune diseases occurring in children. In an autoimmune disease, a person's immune system targets his/her own organ systems resulting in a disease. The most common childhood arthritis condition is Juvenile Idiopathic Arthritis, a term describing chronic arthritis in children under 16 years of age. The exact causes of JIA are not known. Genetic factors appear to play a a major role in predisposing a child to develop arthritis. The purpose of this study is to identify genes that may cause JIA. Identifying genes involved in JIA might improve our understanding of JIA and other chronic arthritis in children. This will also improve the treatment of arthritis and related conditions.
The goal is to enroll 1000 individuals, including children with juvenile arthritis, as well as controls. The controls will consist of healthy individuals, as well as children with other autoimmune diseases. Participants must be willing to donate approximately 1 tablespoon of blood to the study one time. In some instances, we will use saliva instead of blood, when the yield of blood is small. Some children undergo injection of medicine into the affected joints as part of their treatment. If they are willing, the joint fluid will be saved for research instead of being discarded. No joint injections or aspiration will be done specifically for the study. In addition, we will ask subjects to separately consent to provide a stool sample. This sample will be used to look at bacteria in the gut. Some of these bacteria in newly diagnosed children will be linked with genetic and immune bio-markers. We are hoping that this information will help us determine the exact cause of JIA.
The blood will tested for a variety of genes. In addition, any extra blood and joint fluid will be stored for future testing. Additional information will be gathered from the medical chart. This will include demographic information like age, gender and race. Clinical information such as type of arthritis, age at onset, response to medications, evidence of damage from arthritis, family history and results of any radiographic or laboratory testing will also be collected.
Aims include:
[1] ascertain cases of JIA and related diseases from patients seen at the pediatric rheumatology clinics at Emory Children’s Center;
[2] collect phenotypic information and biological material from these patients, first or second degree relatives of subjects in multiplex families and control subjects;
[3] identify epidemiological, biological and genetic and factors involved in susceptibility to JIA and related diseases.
PACMAN: Immunological Characterization of Pre-Clinical Autoimmunity in Pediatric Patients
A diverse group of antibodies is required to protect against infections. Because this group is generated randomly, self-reactive B cells are common. In healthy individuals these anti-self B cells are tightly regulated and do not produce antibodies. Failure of this regulation results in autoimmune disease. While studies on mice have provided insight into this process, how it operates in humans (children in particular), is not as well understood. The primary purpose of this study is to compare the immune phenotype, function, and specificity of B lymphocytes from different developmental stages in pediatric patients with autoimmunity to B cells of adults with autoimmunity as well as healthy controls.
The information derived from this study may help us to better understand the immune system and the biomarkers that eventually lead to the clinical progression of disease in some individuals and not in others. We predict that in patients with autoimmunity, core defects in B cells result in a failure of immune regulation at certain points. These checkpoints are central during infectious disease and maintaining normal health. Understanding when and how immune regulation fails will provide us a better understanding of the autoimmune disease process and potential points of treatment intervention.
JAMS: Joint Associated Mechanical Sounds
Juvenile Idiopathic Arthritis (JIA), an autoimmune disease of the joints, is one of the most common chronic illness of children. JIA is nearly as common as juvenile diabetes, meaning that it affects more children than sickle cell anemia, cystic fibrosis, hemophilia and the muscular dystrophies combined.
Fortunately, JIA is treatable with early intra-articular steroid injections and biologic medications. However, these treatments have several side-effects ranging from GI upset all the way to potentially increasing the risk of cancer. It is with that in mind that the need for ongoing monitoring, and personalized treatment regimens becomes clear.
Currently, we rely on a combination of imaging, physical exam, lab tests, symptoms and clinician’s judgement to monitor JIA. There is not a specific biomarker used to easily monitor the disease progression. The goal of our research is to discover a new biomarker for monitoring joint health. In order to do so, we are listening to the joints. We have all heard our joints crack and pop - our project is discover-ing the meaning behind those noises. Particularly, we are recording the sounds emitted by patients’ joints and correlating that with their clinical scenario.
For the study, a customized, wearable sensing hardware was designed specifically for pediatric patients using commercially available, off-the-shelf (COTS) microphones, sensors, and electronics. The use of COTS will greatly accelerate the process of hardware development, while reducing cost, and will allow for rapid data collection.
The hardware consists of small, high-quality microphones (both piezoelectric contact and electret microphones) and accelerometers connected via flexible wires to recording equipment and a PC (or digital recorder). Example measurements from a knee joint are shown in the figure.
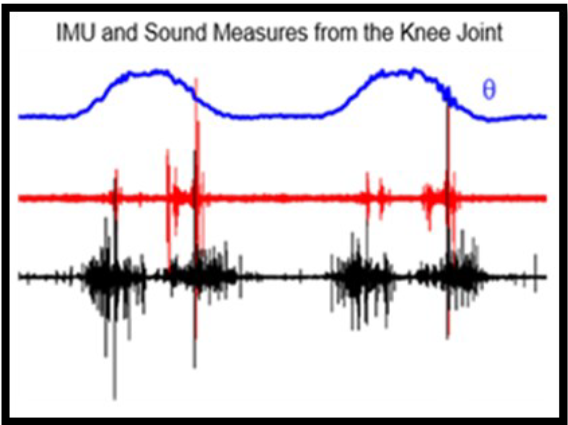
The top plot (blue line) represents the angle of the knee from full flexion to full extension. The next two plots (red and black) are the sounds we record. This data was obtained with existing sensing hardware at the Inan Research Lab and is analogous to our development plans for this study. These microphones and sensors will be attached, temporarily, near various joints on the surface of the skin with COTS adhesives and wearable textile wraps.
Ultimately, we plan to use these sounds in two ways: to easily monitor JIA and to inform a feedback-controlled, personalized treatment schedule.
Primary Investigator: Dr. Sampath Prahalad

Senior Research Lab Coordinator: Lori Ponder
Research Specialist: Talia Gergely

Laboratory contact number: (404) 727- 3861
Discovery Students (from Emory School of Medicine)
- Emily Ferrell (2012)- Characteristics of rheumatoid factor and CCP positive JIA
- Lauren Lange (2013)- The Association between oral hygiene and the development of Childhood Onset Rheumatoid Arthritis
- Katelyn Burges (2014)- Replication of oligoarticular and polyarticular JIA risk variants in other JIA subtypes
- Amanda Huey (2015)- Epidemiological of childhood systemic lupus erythematosus
- Nicole Treadway (2017-2018)- Gene Expression profiling of new onset Juvenile idiopathic arthritis
- Brandon Estroff (2018)- Seasonality of birth and onset of juvenile idiopathic arthritis
Previous Lab Members:
-
Nirja Acharya (Currently in Pediatric Residency) 2011-2012
-
Merlyn Kaalla (Currently in osteopathic school) 2011-2012
-
Christina Tejeda (Currently in Colombia medical school, NY) 2011-2014
-
Gabriel Wang (Applying for medical school) 2011-2014
-
Yelena Shabelnik (Currently in osteopathic school) 2012-2014
-
Se Ryeong Jang (MPH program) 2014-2015
-
Gabrielle Guefen (Currently in PT school) 2014-2016
-
Kimi Chan (Currently in Medical School) 2015-2017
Physicians at the Jingle Bell 5K Arthritis Foundation Run:


Researcher's in the lab:
Familial autoimmunity
Since fellowship, I have been involved in understanding familial factors involved in autoimmunity. I co-authored the largest report of twins concordant for JIA. Our work on increased prevalence of autoimmunity in relatives of JIA cases supported the hypothesis that clinically distinct autoimmune phenotypes share common genetic susceptibility factors (1), which has been recently confirmed by the large genomic studies including the Immunochip studies. We provided for the first time reliable estimates of increased risk of JIA among siblings and first cousins of probands with JIA (3). We recently demonstrated that relatives of cases with JIA were enriched for inflammatory arthropathies, whereas relatives of cases with lupus were enriched for lupus (4). These contributions have enhanced our understanding the genetic epidemiology of JIA.
1. ***Prahalad S, Shear ES, Thompson SD, Giannini EH, Glass DN. Increased prevalence of familial autoimmunity in simplex and multiplex families with juvenile rheumatoid arthritis. Arthritis Rheum 46(7):1851-6, 2002.
2. *Prahalad S, O'Brien E, Fraser AM, Kerber RA, Mineau GP, Pratt D, Donaldson D, Bamshad MJ, Bohnsack JF. Familial aggregation of juvenile idiopathic arthritis. Arthritis Rheum 50(12):4022-4027, 2004.
3. *Prahalad S, Zeft AS, Pimentel R, Clifford B, McNally B, Mineau GP, Jorde LB, Bohnsack JF. Quantification of the familial contribution to juvenile idiopathic arthritis. Arthritis Rheum. 62(8):2525-9, 2010. PMC2921017.
4. Prahalad S, McCracken CE, Ponder LA, Angeles-Han ST, Rouster Stevens KA, Vogler LB, et al. Familial autoimmunity in the Childhood Arthritis and Rheumatology Research Alliance registry. Pediatr Rheumatol Online J 14(1):14, 2016. PMC4785640
Genetics of JIA
JIA is a complex trait influenced by both genetic and environmental factors. My career vision has been to determine who gets JIA and why? Over the past 15 years I have been investigating genetic factors in JIA using various approaches including case-control association studies (5) and genome wide association studies (7,8) These have been facilitated by the ascertainment and careful phenotyping of over 1200 JIA cases and over 1000 controls. These studies illuminate the variety of my contributions to the genetics of JIA. The Immunochip manuscript (7) is one of the most important contribution to the field of JIA genetics to date. I have recently also been involved in gene expression studies (8) to go beyond genetic discoveries.
5. *Prahalad S, Hansen S, Whiting A, Guthery SL, Clifford B, McNally B, Zeft AS, Bohnsack JF, Jorde LB. Variants in TNFAIP3, STAT4 and C12ORF30 loci are associated with multiple auto-immune diseases, including Juvenile idiopathic Arthritis. Arth Rheum 60 (7) 2124-30, 2009. PMC3104295
6. ***Hinks A, Cobb J, Marion MC, Prahalad S, Sudman M, Bowes J, Martin P, Comeau ME, Sajuthi S, Andrews R, Brown MR, Chen WM, Concannon P, Deloukas P, Edkins S, Eyre S, Gaffnew PM, Guthery SL, Guthridge JM, Hunt SE, James JA, Keddache M, Moser KL, Nigrovic PA, Onengut-Gumuscu S, Onslow ML, Rose CD, Rich SS, Steel K, Wakeland EL, Wallace CA, Wedderburn LR, Woo P, Boston Children’s JRA Registry, BSPAR group, CAPS, CHARMS, GKJR, JIA gene expression study, NIAMS JIA genetic Registry, TREAT study, UKJIAGC, Bohnsack JF, Hass JP, Glass DN, Langefeld CD, Thomson W, Thompson SD. Dense genotyping of immune loci using ImmunoChip identified 14 new susceptibility loci for juvenile idiopathic arthritis. Nature Genetics, 45(6):664-9, 2013. PMC3673707
7. Hinks A, Bowes J, Cobb J, Ainsworth HC, Marion MC, Comeau ME, Sudman M, Han B; Juvenile Arthritis Consortium for Immunochip., Becker ML, Bohnsack JF, de Bakker PI, Haas JP, Hazen M, Lovell DJ, Nigrovic PA, Nordal E, Punnaro M, Rosenberg AM, Rygg M, Smith SL, Wise CA, Videm V, Wedderburn LR, Yarwood A, Yeung RS, Prahalad S, Langefeld CD, Raychaudhuri S, Thompson SD, Thomson W. Fine-mapping the MHC locus in juvenile idiopathic arthritis (JIA) reveals genetic heterogeneity corresponding to distinct adult inflammatory arthritic diseases. Ann Rheum Dis 76(4):765-72, 2017. PMC5530326
8. Mo A, Marigorta UM, Arafat D, Chan LHK, Ponder L, Jang SR, Prince J, Kugathasan S, Prahalad S, Gibson G. Disease specific regulation of gene expression in a comparative analysis of juvenile idiopathic arthritis and inflammatory bowel disease. Genome Med, 10(1):48; 2018. PMC6020373
Phenotype of JIA
JIA is a heterogeneous group of chronic arthropathies with varied age of onset. I have been involved in efforts to characterize the phenotype of JIA. An early project I was involved in identified age specific effects of HLA alleles associated with JIA (9) and I participated in data analysis. In order to better understand the biology of JIA, I have investigated serological factors including cytokines (10) and anti-cyclic citrullinated peptide antibodies (11). We have also reported on the largest cohort of African American children with JIA demonstrating that the phenotype of JIA is distinct in this population (12). These exemplify the importance of careful phenotyping to understand the biology of JIA.
9. ***Murray KJ, Moroldo MB, Donnelly P, Prahalad S, Passo MH, Giannini EH, Glass DN. Age specific effects of JRA-associated HLA alleles. Arthritis Rheum 42(9):1843-53, 1999.
10. Prahalad S, Martins TB, Tebo A, Whiting A, Clifford B, Zeft AS, McNally B, Bohnsack JF, Hill HR. Elevated serum levels of soluble CD154 in children with juvenile idiopathic arthritis. Pediatr Rheumatol Online J, 6 (1):8, 2008. PMC2430568
11. Tebo AE, Jaskowski TD, Davis WK, Whiting A, Clifford B, Zeft AS, McNally B, Hill HR, Bohnsack JF, Prahalad S. Profiling anti-cyclic citrullinated peptide antibodies in patients with juvenile idiopathic arthritis. Pediatric Rheumatology Online Journal, 10(1):29, 2012. PMC3490766
12. Fitzpatrick L, Broadaway KA, Ponder L, Angeles-Han ST, Jenkins K, Rouster-Stevens K, Pelajo CF, Conneely K, Epstein MP, Benitez-Lopez J, Vogler LB, and Prahalad S; CARRA Registry Investigators. Phenotypic Characterization of Juvenile Idiopathic Arthritis in African American Children. J rheumatology 43(4):799-803, 2016. PMC4818667
Childhood onset rheumatoid arthritis
Rheumatoid arthritis (RA) is one of the most common chronic inflammatory arthropathies. Years ago I published a meta-analysis of CCR5-Δ32 polymorphism and RA (13). More recently, I have been investigating factors influencing the development of rheumatoid factor and cyclic citrullinated peptide antibody positive arthritis in childhood. This rare subset of JIA phenotypically resembles adults with RA, suggesting that RF/CCP positive JIA reflects childhood onset of RA. I led an international collaboration to assemble the largest cohort of RF/CCP positive JIA and showed there is a hierarchy of HLA DRB1 alleles in children with CORA (14). We have also shown the utility of a weighted genetic risk score towards susceptibility to childhood onset RA (15). Recently we have shown that childhood onset RA is genetically similar to RA in adults (16). These are among the most focused studies of this phenotype.
13. ***Prahalad S. Negative association between the chemokine receptor CCR5-Δ32 polymorphism and rheumatoid arthritis: a meta-analysis. Genes and Immunity. 7(3): 264-8, 2006. PMC3104293
14. Prahalad S, Thompson SD, Conneely K, Jiang Y, Leong T, Prozonic JL, Brown MR, Angeles-Han S, Vogler LB, Kennedy C, Wallace C, Wise C, Punaro M, Reed A, Park J, Mellins E, Zeft A, Bohnsack J, and Glass DN. Hierarchy of risk of childhood onset rheumatoid arthritis conferred by HLA-DRB1 alleles encoding the shared epitope. Arthritis Rheum 64(3):925-30, 2012. PMC3276774
15. Prahalad S, Conneely KN, Jiang Y, Sudman M, Wallace C, Brown MR, Ponder L, Pichavant MR, Zwick ME, Cutler DJ, Angeles-Han ST, Vogler LB, Kennedy C, Rouster-Stevens K, Wise C, Punaro M, Reed AM, Mellins E, Bohnsack J, Glass DN, and Thompson SD. Susceptibility to Childhood onset rheumatoid arthritis: investigation of a weighted genetic risk score that integrates cumulative effects of five variants at five genetic loci. Arthritis Rheum, 65(6):1663-7, 2013. PMC3683854
16. Hinks A, Marion MC, Cobb J, Comeau ME, Sudman M, Ainsworth HC, Bowes J, Juvenile Idiopathic Arthritis Consortium for I, Becker ML, Bohnsack JF, Haas JP, Lovell DJ, Mellins ED, Nelson JL, Nordal E, Punaro M, Reed AM, Rose CD, Rosenberg AM, Rygg M, Smith SL, Stevens AM, Videm V, Wallace CA, Wedderburn LR, Yarwood A, Yeung RSM, Langefeld CD, Thompson SD, Thomson W, Prahalad S. The Genetic Profile of Rheumatoid Factor-Positive Polyarticular Juvenile Idiopathic Arthritis Resembles That of Adult Rheumatoid Arthritis. Arthritis Rheum, 70(6):957-62, 2018. PMC5984672.
Collaborative studies in the genomics of inflammatory diseases:
Although improved genomic technologies and the fall in costs have played a major role, the explosion in genomic discoveries requires large cohorts of well-phenotyped subjects. I have been part of multiple collaborations of autoimmune phenotypes including psoriasis (17), biomarkers in oligoarticular and RF-negative polyarticular JIA (18), systemic onset JIA (19), and targeted next generation sequencing in inflammatory bowel disease (20).
17. ***Nair PR, Duffin KC, Helms C, Ding J, Stuart PE, Goldgar D, Gudjonsson JE, Li Y, Tejasvi T, Feng BJ, Ruether A, Schreiber S, Weichenthal M, Gladman D, Rahman P, Schrodi SJ, Prahalad S, Guthery SL, Fischer J, Liao W, Kwok PY, Menter A, Lathrop GM, Wise CA, Begovich AB, Voorhees JJ, Elder JT, Krueger GG, Bowcock AM, Abecasis GR. Genome-wide scan reveals association of psoriasis with IL-23 and NF-kB pathways. Nature Genetics. 41(2):199-204, 2009. PMC2745122.
18. Mor-Vaknin N, Rivas M, Legendre M, Mohan S, Yuanfan Y, Mau T, Johnson A, Huang B, Zhao L, Kimura Y, Spalding SJ, Morris PW, Gottlieb BS, Onel K, Olson JC, Edelheit BS, Shishov M, Jung LK, Cassidy EA, Prahalad S, Passo MH, Beukelman T, Mehta J, Giannini EH, Adams BS, Lovell DJ, Markovitz DM. High Levels of DEK Autoantibodies in Sera of Patients With Polyarticular Juvenile Idiopathic Arthritis and With Early Disease Flares Following Cessation of Anti-Tumor Necrosis Factor Therapy. Arthritis Rheumatol 70(4):594-601, 2018. PMC5876119
19. Arthur VL, Shuldiner E, Remmers EF, Hinks A, Grom AA, Foell D, Martini A, Gattorno M, Özen S, Prahalad S, Zeft AS, Bohnsack JF, Ilowite NT, Mellins ED, Russo R, Len C, Oliveira S, Yeung RSM, Rosenberg AM, Wedderburn LR, Anton J, Haas JP, Rösen-Wolff A, Minden K, Szymanski AM; INCHARGE Consortium, Thomson W, Kastner DL, Woo P, Ombrello MJ. IL1RN variation influences both disease susceptibility and response to recombinant human interleukin-1 receptor antagonist therapy in systemic juvenile idiopathic arthritis. Arthritis Rheumatol 70(8):1319-1330, 2018. PMC6105455
20. Chen JS, Hu F, Kugathasan S, Jorde LB, Nix D, Rutherford A, Denson L, Watkins WS, Prahalad S, Huff C, Guthery SL. Targeted Gene Sequencing in Children with Crohn's Disease and Their Parents: Implications for Missing Heritability. Genes3 (Bethesda).8(9):2881-8, 2018. PMC6118318
*indicates >50 citations; ***>100 citations
A complete list of papers (n = 113) is available at: http://www.ncbi.nlm.nih.gov/pubmed/?term=prahalad+S